
68% of COVID-19 deaths during the first year of the pandemic were adults in low socioeconomic positions
University of South Florida epidemiologist Jason Salemi’s research confirmed associations between COVID-19 mortality rates and socioeconomic position, gender, ethnicity and race.
Salemi’s research shows:
- The mortality rate of low SEP adults is five times higher when compared to high SEP adults, and the mortality rate of intermediate SEP adults is two times higher.
- White women make up the largest population group considered high SEP. In contrast, nearly 60 percent of Hispanic men are in a low SEP.
- When compared, the mortality rate of low SEP Hispanic men is 27 times higher than high SEP white women.
“The degree to which it takes a toll on communities is very unevenly distributed and we wanted to call attention to that issue,” Salemi said.
Reminder that crackers started storming state capitols demanding lockdowns end about a week after news reported covid was harming black people at far greater rates than anyone else.
The “return to normal” was driven by complete disregard to the lives of low wage workers and outright racism.
But I’m sure things are great now that the “pandemic is over”. Genocide Joe and the party of science wouldn’t lie to you. Capitalism wouldn’t just sacrifice workers like that, right?
The pandemic is class warfare

It’s why nations with powerful communist parties kept covid rates down for as long as possible.
Giving a shit about covid is a big part of solidarity that a lot of people seem to have given up on.
not just solidarity, I’d liken it to climate change at this point
I’ve heard many stories both here and on
 about people who’ve NEVER CAUGHT COVID before getting it, getting long-COVID, and even dying of it
about people who’ve NEVER CAUGHT COVID before getting it, getting long-COVID, and even dying of itit feels like a probability game, except it’s mutating into like 20 strains every second so there could be a 100% probability that it eventually fucks everyone over
The fact that all-cause mortality was ~20% higher during the year of 2022/23 lends credence to thisthe operating assumption, including on hexbear, is that if you were unaffected until now you’re good, and that’s not really true
I’ve been operating under the assumption that we’re all playing the ‘How many Covid infections does it take to kill you, either directly or indirectly?’ game, and I don’t think I’m alone in that in this comm, at least.
Russian roulette with viruses
Lol, yeah pretty much. Though I’ve stopped using that phrase because it feels too much like that lib thing of pointing at the horrors of capitalism and calling it communism. 😅
Edit: Maybe more like Pokemon with viruses.

I 100% agree. I wish people still cared. I’m high risk for multiple reasons and very few people seem to understand why I’m still taking heavy precautions.
I’m not high risk AFAIK but I mask whenever indoors or among people outdoors because I don’t need fucking long covid.
And yet people will think we’re the weirdos for wanting to put in the bare minimum effort to avoid permanent brain, lung, or heart damage.
We bear witness to the power of normalization
I just went to a physical and I had been feeling shitty, so I asked them for a covid test. The HOSPITAL told me they dont do covid tests, I had to get a retail one. I paid $23 for just two tests. And its not like I get paid vacation if I test positive. I work in a kitchen. And my doctors visit was $300 anyways cuz I dont have insurance. I’m convinced that workers are being forced into risky decisions cuz they dont have the money to survive this shit. Maybe cut military aid to Ukraine and Israel and use that to pay for everyones healthcare and give out some federally funded sick days? Idk, just a thought
A hospital doesn’t do COVID tests? What the fuck?
I was already having a really bad day mentally, this isn’t helping…
Sorry you are dealing with all this, I hope you feel better soon.
Yeah, this last summer we changed testing and reporting requirements. Check out this graph for US hospitalizations. Source is from: https://nitter.poast.org/maolesen
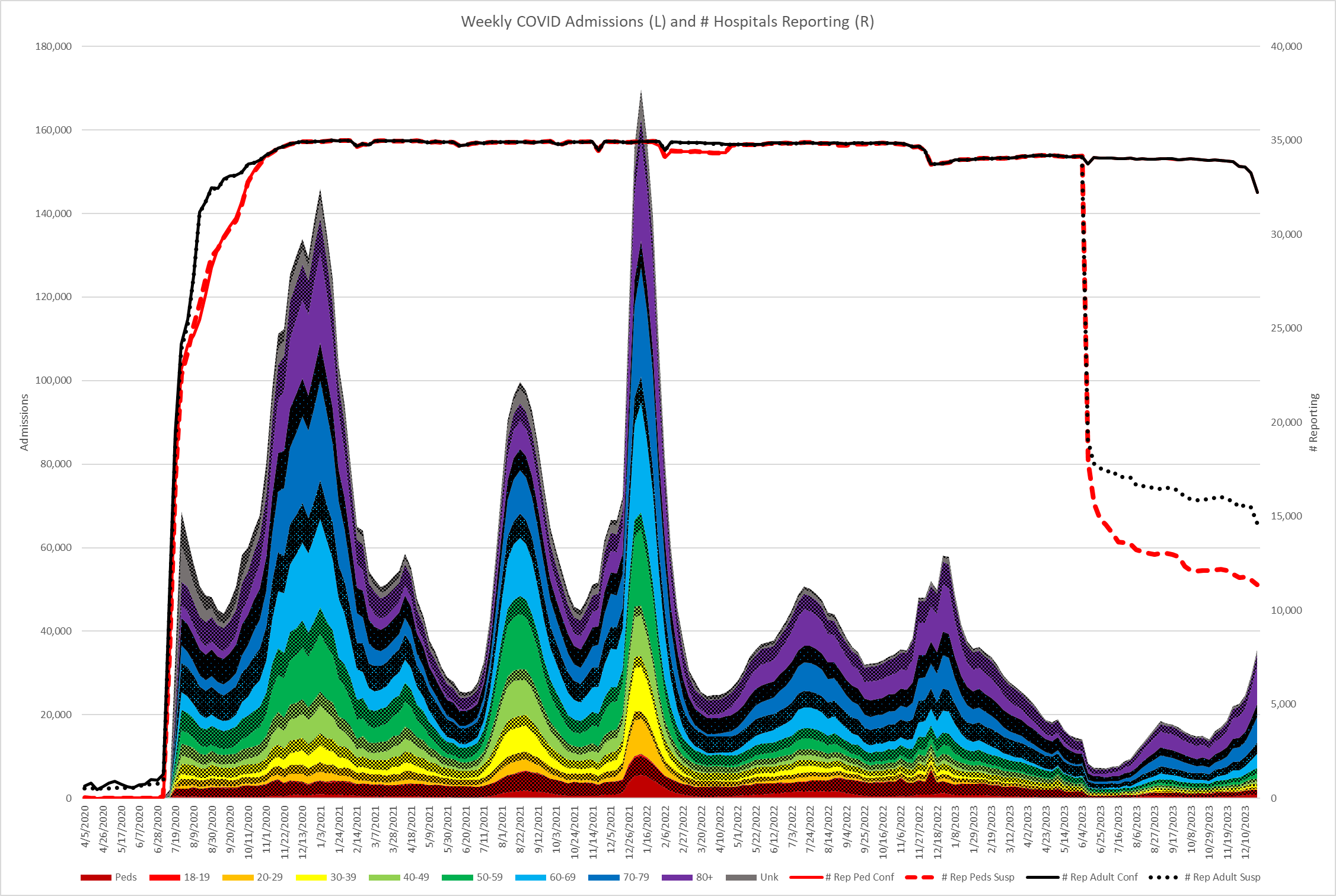
Can you spot the time when covid testing and reporting requirements were dropped? The top dotted red line is the amount of hospitals testing suspected cases. When people say it’s better now keep in mind that we aren’t measuring the same way, we are straight up testing less. We shaved off a substantial percentage of covid hospitalization cases this way.
Ooooooh I believe it. Biden CDC has been worse then the bad orange man’s.
Covid is a class issue.
I just read a paper on where covid came from in my homecountry Finland. The entire spread of it was from tourist spots in three other European countries where the upper classes like to vacation and did during the first years. One ski resort in Austria seeded one wave alone here basically. Not a single case that spread further ever arrived here from Wuhan for example, the spreading was all done by the high income brackets from their vacationing.
Now the brunt of it is beared by the service workers, the labor aristroes are happily cushioned in their remote work and it is still them who keep bringing new variants in, those who say “I need to travel for mental health” or whatever.
Covid is a class consciousness issue on a very real level, it’s the working class that dies from it.
Another example of a class which benefits from the destruction of public health measures is petit bourgeois shop owners, whose businesses cannot function under conditions of reduced in-person travel
 Healthcare, please
Healthcare, pleaseRemoved by mod
Please stop posting that imgur album of
 nonsense.
nonsense.make me
fair enough carry on
Until the secretive authoritarian US government opens up fort detrick and allows a full investigation we will never know the truth. What are they hiding?
And like always, never forget that this was a US bioweapon!
I can’t access the image, but it is kind of funny that the US funded gain-of-function experiments we were doing with coronaviruses (or at least experiments very similar to gain of function), were taking place in North Carolina. They collaborated with the Wuhan institute because that’s who you would collaborate with if you wanted to research SARS. Right wingers bang on about this issue because they can do the “China bad” thing, but the research they are blaming for creating covid would have been done in North Carolina.
The conclusion, of course, is that since the outbreak didn’t start in North Carolina, obviously this research wasn’t responsible for covid.
But if Covid did start in the US, how quickly does anyone think we would have detected it? It would have just been a mystery cold from hell until it got into a long term care home. It was in China for a month or two before they detected it, and unlike the US, they were actively monitoring for SARS.
So were there any mysteriously deadly pneumonia outbreaks occuring in North Carolina in late 2019? Yes. Yes there were. In at least a couple of long term care homes. We never investigated any of those outbreaks to see if there was SARS present… because why bother? It started in China.
Americans want to blame China for COVID but if something similar starts up, say, in the deplorable conditions of a factory pig farm in Arkansas, practically every non-vegan American would become incredibly indignant over accepting any blame.
It would be more like if China was running a pig operation at an American farm, and then a pandemic hit, and everyone blamed America lol
I can’t access the image
I managed to find it in their history, here it is: https://imgur.com/a/CRwan3n
According to him the outbreak did start in the US, but it was less contagious at the start. Hence the outbreaks in Virginia retirement homes and throughout US schools and in vapers, but not having mass-population contagion yet
So were there any mysteriously deadly pneumonia outbreaks occuring in North Carolina in late 2019?
The “mysterious” US outbreaks start from June 2019 into November 2019, well before the official date of the Chinese outbreak.
There was also that weird Spanish sewer sample from May 2019? or March 2019 I forget. But that one could maybe be a freak/unrelated
An Imgur link was detected in your comment. Here are links to the same location on alternative frontends that protect your privacy.
The exposure is next level. Schools, daycares, healthcare settings too, clearly jobs where there are a lot of women as well. Pretty sure the response would look different if more tech bros were dying or getting longcovid from this. Sadly we might be getting there though.
And public health messaging has truly been motivated by the capitalists on this.
We currently have the tail-end covid and we had an electrician come over yesterday and my partner told him that we are likely still not good to be around. The guy replied with “Yes, but I am vaccinated 4 times”. My partner replied with “I am 5 times and still have been sick for almost two weeks now, would you like a mask?”. He was happy to take the mask.
It was still risky for him, but they are sent to these apartments by the landlords who employ them and nobody cares to protect the workers.
Biggest issue is that these workers clearly trust public health enough that they really think they are protected now. What will this do to that trust, why is anyone surprised that anti-vax sentiments are on the rise? It’s a symptom of this.
Pretty sure the response would look different if more tech bros were dying or getting longcovid from this
I know a lot about long-COVID, and roughly 80% of LC sufferers on reddit are white (which is parity for reddit, being 80% white as a whole)
Latinos were overrepresented at something like 10% while being only 3% of reddit as a whole
I think a lot of people are developing long-covid symptoms which are “mild” enough that we don’t hear about them
Biggest issue is that these workers clearly trust public health enough that they really think they are protected now. What will this do to that trust, why is anyone surprised that anti-vax sentiments are on the rise?
The biggest elephant in the room on Hexbear is that every single thing the vaccine was supposed to do was gradually walked back step by step until it’s now AT BEST a slight band-aid that doesn’t even stay on properly.
The vaccine is almost useless, the illness is a bioweapon and radical 1960s style hardcore hippie organizing is the only way to even stand a chance at eradicating it (I was banned from for this last line)The vaccine does significantly reduce the risk of a slow and painful death to Lungs Broken.
Removed by mod
You’re kind of running a survivorship and confirmation bias there, though. Vaccines aren’t instantly effective, so if someone dies shortly after getting vaccinated, that’s not proof the vaccine didn’t work. And of course someone isn’t going to say the vaccine didn’t prevent their death if they died, and they wouldn’t say it prevented their death regardless because they still got sick. We’ve known for years the vaccines don’t stop sickness, they just reduce the lethality of infection.
Removed by mod
Removed by mod
Sadly we might be getting there though.
how? don’t they mostly work from home?
The push for return to office. At least here I am hearing about more and more sick tech workers, the whole “our entire office is sick”-thing. Not everyone will come out of that ok.
Statistically the push for in person stuff will raise their exposure too. They are working class, and can lose their protection on a whim, many have already lost it.
The amount of finance shenanigans the capitalist class has going on around in the use of these office buildings and other in-person infra is huge. And we spend a lot more when we have to leave our homes. Travel, eating out, clothing. They want the high earners out there, consuming and getting sick.
It’s NOT a probability thing of “they’re more exposed so they’re more likely to get it”. It’s rather “they’re more exposed so they’re breathing in 1000x more spike protein/virus, and 1000 is a bigger number than 1”
But doesn’t that manifest as a higher probability of getting it? Or do they end up getting like, mini-Covid?
Removed by mod
So it IS basically mini-Covid. Wild
Removed by mod
My understanding is that the spike protein can bind to pretty much every cell in our body, and our immune system will react to it, which is how the vaccines work. The danger would come from the constant triggering of the immune system when exposed to the spike protein, but if it’s not attached to a virus it won’t replicate in our body, and that limits the damage it can do.
Our t-cells destroy infected cells so a controlled dose in the form of a vaccine is quite a bit safer than the live virus, but if it attaches to a vital organ it can still cause damage depending on how nuts our bodies immune response is. If there is any spike protein shedding from people through breath it would likely be a limited amount and our bodies shouldn’t have a problem clearing it because it won’t reproduce and won’t be putting out chemical signals that allow it to avoid an immune response while actively reproducing 1000x like covid does. The amount of damage covid does seems to be dependent on how much you are exposed to, and the less virus you get exposed to the better.
When it’s attached to the actual SARS virus it can do a ton of other shit like turn your cells into a covid factory, infect T-Cells and get in bone marrow and crazy ass shit like that. It’s getting into places our body has a hard time clearing and staying there. People infected might never clear the virus at this point, and it could be like chickenpox, EBV, or herpes and likely has a chance to come back whenever the immune system is stressed. Any abnormal levels of spike protein is likely due to a persistant infection. They are finding traces of them in the organs of people who died several months or years after getting infected.
People researching the virus mutations believe a lot of them come from people who never clear the virus and whatever mutations the variant they harbor is combining with the dominant variant in circulation, and viola a new world dominating virus is born.
The Cuban vaccines, which seem to be extremely successful, target an RBD receptor instead of the spike protein. It would be interesting to see how the cuban population compares to the US when it come to long covid and these types of symptoms.
Our t-cells destroy infected cells so a controlled dose in the form of a vaccine is quite a bit safer than the live virus
agreed, but one possible gripe is that the Western vaccines are not a controlled dose of spike protein, but rather an instruction book on how to make spike protein for your body’s cells. It kinda feels like it could be giving a monkey an AK-47, there’s just so many more steps/variables there than with a normal vaccine
People researching the virus mutations believe a lot of them come from people who never clear the virus and whatever mutations the variant they harbor is combining with the dominant variant in circulation, and viola a new world dominating virus is born.
That’s probably a source but I doubt it’s the main one. Since the vaccines don’t prevent infection, every vaccinated person is still a walking covid recombination reservoir in 2024. The impact of people who “can’t clear” the virus feels insignificant, numerically.
I also think that covid symptoms have little to do with covid infection, and much more to do with spike sensitivity of the individual. There are lots of people, even pre-vaccine, who just don’t feel anything from covid. Then there are people who have a bad month if they go outside in public even for a minute.
There was a girl back in 2020, who was COVID positive for over a month. She was pretty fine symptom-wise
If there is any spike protein shedding from people through breath it would likely be a limited amount and our bodies shouldn’t have a problem clearing it because it won’t reproduce and won’t be putting out chemical signals that allow it to avoid an immune response while actively reproducing 1000x like covid does.
True. But spike protein is 1000x smaller than the virus. Whatever your mask is doing for blocking the virus, it’s much more useless when it comes to airborne spike.
That’s probably a source but I doubt it’s the main one. Since the vaccines don’t prevent infection, every vaccinated person is still a walking covid recombination reservoir in 2024. The impact of people who “can’t clear” the virus feels insignificant, numerically.
Unfortunately, from the researchers I’m following, It’s actually looking like viral persistance quite common. Maybe it’s why virus levels in wastewater always remain high?
I also think that covid symptoms have little to do with covid infection, and much more to do with spike sensitivity of the individual. There are lots of people, even pre-vaccine, who just don’t feel anything from covid. Then there are people who have a bad month if they go outside in public even for a minute.
Evidence is stacking up that after the acute period symptoms are probably from immune dysregulation. Basically covid causes our immune system to keep attacking our body long after the acute infection, causing inflammation and long covid systems, and it’s more evidence pointing to a persistant viral reservoir in the body.
Blood tests can show which antibodies we have and the ones produced after vaccination are distinct from the one created after infection from the virus. If it was just the spike protein alone causing problems we could determine that with a blood test. But none of the sources I follow have shown any research on this.
An Imgur link was detected in your comment. Here are links to the same location on alternative frontends that protect your privacy.

Death to america, death to capitalism
We will remember this in November.
I’m ready to
 right now!
right now!
Our frontline heroes 💀
I’m glad the data is there, but also it’s unsurprising that people who have jobs that expose them more (both from clients and other employees), are in more financially precarious positions so are more likely to ignore mild symptoms to get to work, and have access to worse healthcare… Yeah.
This is true but the mortality rate has nothing to do with race biologically
it has to do with stress and maybe inherited markers of stress
African people in Africa are highly protected from COVID
The disparity of outcomes in race seems to have more to do with the US have more to do with the burden of systemic racism and more people as a percentage of their population being poor or working class, so high risk jobs, greater environmental stressors, lack of access to adequate healthcare, along with the healthcare system being racist.
The better outcomes reported in Africa seem to be from under-testing, this study states that about 50% of Africans who got a confirmed covid infection have long covid, which probably means they were missing a lot of people with covid testing.
You can see how excess deaths compare to actual covid cases in South Africa here: https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(22)00425-9/fulltext
Like most other places around the world, excess deaths skyrocket during big covid waves.
On the contrary, we observed that long COVID was more frequent in Northern (47.73%) or Southern (48.89%) African countries when compared to Eastern ones (5.06%)
(Western Africa has 17%)
The studies were mainly made in Egypt (12/25 = 48%), their mean age was 42 years (range 7–73)
That 50% figure is for North Africans and Whites, not Black Africans (who have a 10% Long-Covid symptom frequency when east/west are averaged)
deleted by creator